









A brief overview of the appropriate use of antibiotics in paediatric dentistry.

Antibiotics are used for the prophylactic and therapeutic treatment of children in dental practices. Prophylactic antibiotics are prescribed in order to prevent diseases in patients with local compromised sites after interventions in the oral cavity, or for the prevention of endocarditis. Therapeutic antibiotics are used in the treatment of complications and infections in the oral cavity. However, since the unwarranted use of antibiotics for the treatment of dental infections in children has been reported, the questions arises whether dentists are adequately informed about the correct use of antibiotics in paediatric dentistry. Furthermore, the misuse of antibiotics may lead to the emergence of antibiotic resistance, one of the major global health problems today.

The incorrect use of antibiotics may be due to inappropriate or unnecessary prescription, incorrect dose or dosage, or inadequate duration of the treatment. The antibiotic therapy should be maintained for at least five days after the point of substantial improvement or resolution of symptoms and should not be stopped immediately after the patient is feeling better. It is crucial to communicate this concept to the patient, in order to prevent potential resistances of antibiotics. It should be mentioned, that in a questionnaire study of 85 dentists conducted in 2019, 23 dentists (17,1%) claimed to treat their patients with an antibiotic therapy with a total duration of 2-5 days (Inchara et al., 2019).
Dentists often prescribe prophylactic antibiotics, attempting to prevent complications and provide the best outcome for their patients. However, prescribing an unnecessary antibiotic in a healthy patient that would most likely not suffer any subsequent infections could potentially lead to antibiotic resistance, and may be detrimental to the health of the patient. It has been shown for example, that for dental extractions, the wound infection rate is below 1%. Therefore, the treatment with prophylactic antibiotics after e.g. extractions would only be justified in case of other indications such as the treatment of immunocompromised patients.
The goal of antibiotic treatment is to use the smallest amount of the agent most effective against the microorganism causing the infection.
The correct approach of antibiotic treatment is the use of the most appropriate antimicrobial agent at the smallest effective amount for an adequate time period. Furthermore, narrower spectrum antibiotics are preferred over broader spectrum antibiotics, and the antibiotic with the least adverse effects as possible should be chosen. To determine the best possible antibiotic, a culture of the causative microorganism is necessary. The exact determination is not always possible, considering the difficulty of obtaining an uncontaminated sample in the oral cavity, which has a diverse flora of microorganisms. However, not all dentists prescribe antibiotics to their paediatric patients. Out of the 85 dentists who took part in the questionnaire survey, 69,4% of them claim to prescribe antibiotics, whereas the remaining 31,6% do not resort to antibiotics (Inchara et al., 2019).
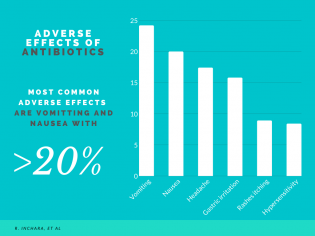 When treating a patient with antibiotics, adverse effects pose a potential risk. As mentioned before, the antibiotic with the least adverse effects will be favoured. However, even frequently prescribed antimicrobials such as penicillin may lead to allergic reactions in 5-8% of patients, or anaphylactic shock in 0,05% of patients. Other adverse effects such as gastric irritation, nausea, vomiting, rashes, itching, headache and depression were associated with penicillin and amoxicillin. The most common adverse effects can be seen in the graph.
When treating a patient with antibiotics, adverse effects pose a potential risk. As mentioned before, the antibiotic with the least adverse effects will be favoured. However, even frequently prescribed antimicrobials such as penicillin may lead to allergic reactions in 5-8% of patients, or anaphylactic shock in 0,05% of patients. Other adverse effects such as gastric irritation, nausea, vomiting, rashes, itching, headache and depression were associated with penicillin and amoxicillin. The most common adverse effects can be seen in the graph.
When calculating the correct dosage of antibiotics for paediatric patients, different factors such as age, weight and severity of the disease must be taken into account. In the earlier mentioned questionnaire study, 25% of dentists based their calculations on age, 43,3% on weight, and 31,8% on the severity of disease (Inchara et al., 2019). However, this leads to the question why an unified approach to the calculation of the correct dosage of antibiotics for paediatric patients has not been introduced. When paediatric patients are treated with antibiotics, they are usually administered through oral route. In case of allergies to tablets or pills, alternative routes of administration such as intravenous or subcutaneous methods must be considered. The research article “Preference of antibiotics in pediatric dentistry” additionally mentions the intra-arterial route as an alternative, though the reality of intra-arterial administration in a dental practice for paediatric patients may prove to be problematic.
When prescribing antibiotics in paediatric dentistry, the dental practitioner faces a set of challenges. First of all, an assessment must be made to determine the necessity of antibiotic therapy in order to prevent unnecessary prescriptions. Furthermore, the correct antibiotic must be chosen, and the dose must be calculated to meet the needs of the patient. Especially in paediatric dentistry, it is essential to make an exact calculation based on the age, weight and the severity of the disease, as compared to general dentistry, where patient doses are usually only based upon the set doses of the national guidelines. Considering the global importance of antibiotic resistance, dentists require guidelines defining the appropriate use of antibiotics in paediatric dentistry.
Generally, it should be in every dentists’ best interest to keep up to date in his/her pharmacological education, in order to optimize patient care and minimize health risks.
The percentages and data used in this blog entry are obtained from:
Inchara, R & Ganapathy, Dhanraj & Pandurangan, Kiran. (2019). Preference of antibiotics in pediatric dentistry. Drug Invention Today. 11. 1495-1498.
This blog entry has been written by German Frentzen and Lennart Prüfer, students of 2nd-year of Dentistry at University CEU Cardenal Herrera




